Three binding factors can limit your physical freedom. The third is seldom discussed or addressed by therapists.
Now you’re reading this journal, can you remember how you arrived here?
Think broad and wide for a moment. I am not only talking about the clicks that were needed to get to this page. I am talking about how you actually arrived at your keyboard. What did you do just before that, and where were you when you decided to get back online?
What I am trying to get to here is that you had to move yourself to come to this post. Very likely, you had to work that keyboard with your fingers and something like a mouse or touchpad to navigate links and tabs. You will have been somewhere else before you sat down at your desk, which means you had to transport yourself somehow to it, either though walking or turning the wheels of your wheelchair.
Did you just realised what your fingers, hands, arms, and shoulders were doing when you scrolled down the page just now? Did you just take a sip from your coffee or tea? Did you move something on your desk five minutes ago – a pen, pencil, or piece of paper perhaps? Are you still breathing?
It’s all about movement and motion – which is what we do just about every second of the day and, I believe, something we have learned to do without thinking about it.
Movement is Life
Like just about any other species, we humans are designed for movement. The human adult body includes 360 joints, which can be found between first 270 bones at birth, which then eventually decreases to 206 as some fuse together later in life. Then we are gifted more than 600 muscles to enable movement of these bones around the joints. By estimation, more than 70% of our body’s weight goes to tissues that are uniquely and primarily tasked with motion and movement.
While that complex but highly effective configuration of anatomical elements can endure much use and even abuse it is, as we all know, not exempt from malfunctioning. Accidents cause us to break bones and damage joints. Misuse, abuse, and disuse of our body eventually leads to structural and mechanical problems, which usually manifest as pains and discomforts. The effects of aging, combined with what might be suboptimal lifestyles, makes us only more prone to such issues.
Normally, we don’t seem to be all that conscious about how we use our body, for as long as it doesn’t protest at what we want it to do. We simply move things and ourselves countless times each day, and typically without much – or any – thought. It’s only when we experience pain or discomfort that we pay attention to what’s actually going on with our physique. It’s usually at this point where we engage a therapist to get ourselves ‘fixed’.
Normal Range of Motion
When you meet a manual or physical therapist to discuss your concern, they will usually examine both your body and how you use it. Because we are well familiar with how our elbows work, let’s take a closer look at how they would observe your movements.
To start with the obvious, we know what a healthy and properly functioning elbow should be able to do. In other words, we know the abilities and limitations of this joint which, if you like, provides something like a baseline for how it should behave.


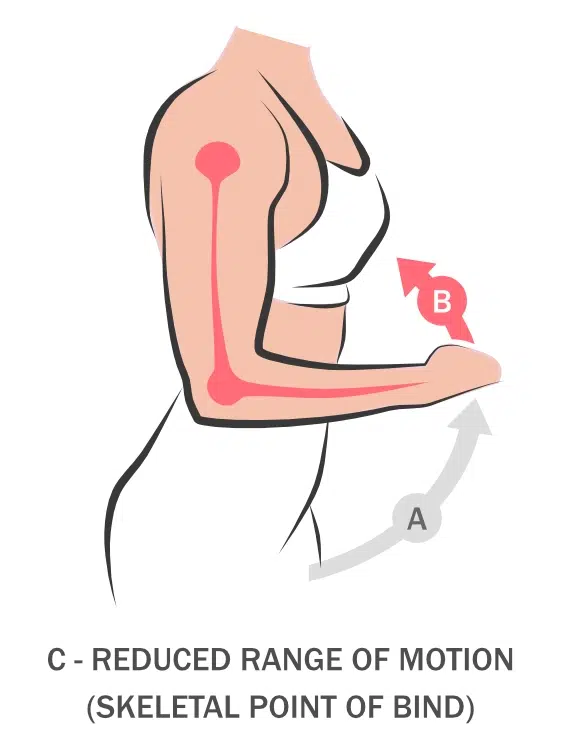
It is simple to determine this for an elbow joint. We know that when it is fully extended, the fingers of that arm should point almost directly toward the ground (A). We also know that from this point the elbow doesn’t allow the forearm to bend backward, simply because its joint isn’t designed that way. In this position, the muscles of the arm should either be relaxed and unengaged or used to carry something.
However, the joint does allow us to raise our hand toward our shoulder, which puts this joint in flexion (B). This movement allows us to touch our face, brush our teeth, or comb our hair for example.
Although muscle mass of the arm plays a role, for an arm to have an optimal Range of Motion (RoM) we should be able to touch our shoulder with our fingers, painlessly and with minimal effort. This may not be possible for those who developed large biceps, which are the muscles that are located at the front of our upper arm.
Reduced Range of Motion (Points of Bind)
Now we understand what movements we can reasonably expect from our elbow joint we can now take another look at what may actually be happening with our concerned client. She may present with a Range of Motion that doesn’t allow her to raise her hand painlessly toward her shoulder which, as we have learned, should be the case normally.
Let’s say that she can raise her arm halfway to a 90-degree angle only. When she tries to raise her hand closer to her shoulder, her upper arm becomes prohibitively painful.
Our examination may start with inspecting the elbow joint as well as the two neighbouring ones – those of the shoulder and wrist (C). We look specifically for conditions such as osteoarthritis, rheumatoid arthritis, gout, bursitis, and tendinitis, which could all play a role in the development of her concern.

Then we focus our attention on the other connective tissues of her arm. We will now identify if muscles and tendons are damaged, too contacted, too weak, or in any other way dysfunctional (D). Because muscles work usually in pairs we will look at her biceps (which is responsible for flexion) as well as her triceps, which are located at the back of her arm (opposite the biceps) and therefore responsible for extension.
For her to raise her hand to her shoulder, her biceps must contract while her triceps must relax. The problem may therefore be caused by a dysfunction on either the front or back of her upper arm, which needs to be understood to avoid working on the wrong muscles or muscle group.
While examining her muscles we also inspect other connective tissues, of which there are seven types in total (including osseous tissue, or bone, and cartilage, on which we already focused earlier. We do not focus on blood, which is also considered a connective tissue). Again, we will be looking for damage caused by injury or incorrect use for example.
Once the likely or actual causes for her arm-raising concerns have been identified we can determine which methods, approaches, and techniques can be used best to solve her problem.
In some cases, more than one type of therapy may be needed, in which case we may refer to a chiropractor, osteopath, rehabilitation specialist, or a surgeon.
Psychological effects on Range of Motion
In most situations, concerns like that of our client are caused by a mechanical issue in joints, muscles, or other connective tissues. However, there is at least one other factor that can influence or affect our client’s range of motion, which is of a psychological nature (E).

This is often the case when the client believes that her range of motion isn’t as optimal as it actually is. Even when nothing seems wrong with the structure and mechanics of her arm (E) she may still be convinced that she cannot raise her hand fully to her shoulder. She may even experience pain when she tries.
Despite the evidence science collected over the last few decades, the relationships between our psyche and our time-space movements remains unclear. At the extremes of the debate, we find those who absolutely believe in a dependency between mind and body on one end, and those who reject the idea simply downright at the other, simply on the basis that research remains inconclusive on the topic.
Based on my own practical experience, my place on this spectrum is on the side of the believers. I do believe that we can think ourselves into postures that are less flexible than they actually should be, or, more poignantly, than they really are. Over the years, many of my clients proved that fear of (re-)experiencing pain can freeze us, which is consistent with what we know about our body’s natural physiological reaction to stressful, frightening, or dangerous events.
Such freezing doesn’t need to be experienced as a whole-body affair; it can also manifest in parts of it. This may precisely be the reason for our client’s arm-related concern. Some underlying psychological issue may prevent her from moving her arm beyond that 90-degree angle further toward her shoulder. In fact, she may even experience pain when she tries to do this, even though there is nothing anatomically and physiologically wrong with her.
Taking our (E)motions Seriously
It is said that every physical injury – or dysfunction – pairs with an emotional response. Yet, from what I learned from my clients over the years, practically none of their previous therapists showed sufficient interest in how trauma affected them psychologically. Apparently, it is often assumed that these paired emotions dissipate once the physical concern has been treated. However, it is my experience that this isn’t necessarily the case.
What seems to have become troublesome is that many therapists are increasingly reliant on rapid client turnover. It is not unusual for therapists to book three clients per hour, usually for financial gains, which consequently allows for no more than approximately 20 minutes hands-on treatment time per session. While this will usually be enough for an experienced therapist to treat a typical physical concern such as C and D above, I believe it isn’t possible to adequately address psychological (emotional) points of bind, such as E, in such short periods of time.
Because most manual and physical therapists will not be licensed to act as psychologists it is certainly true that grey areas exist between the services they can offer and those that are provided by psychologists. Even when clients work with a bodywork therapist and psychologist in tandem, there usually is very little communication and coordination between the three parties, which could otherwise, and quite likely, accelerate the client’s healing.
To narrow and potentially even close these chasms we, bodywork therapists, could take a first step by exploring with our clients about how this third Psychological Point of Bind may manifesting in their healing journey. If the client’s fear for reinjury appears to be significant, it may perhaps be a good idea to have them consider psychological support to address their entire concern – not just what’s literally palpable physically, but also what may be compromising their freedom of movement mentally.
Embracing Advaya’s uniqueness
Whether Psychological Points of Bind really exist is something that still triggers polarised debates between manual and physical therapists. Beyond that conversation, it is equally unclear to those who subscribe to its existence where the responsibilities for the client’s mental care really lie. Ethics come into play when our intentions to help clients regain their physical freedom bump into limitations we cannot resolve professionally.
Years ago, when I established Advaya as a small bodywork practice on New Zealand’s Kapiti Coast, I decided to build its brand on honesty, trust, confidence, and integrity. To stay aligned with these intentions I continued to explore with my clients how Psychological Points of Bind may be at play when they presented their concerns at our clinic. Reality showed that these explorations weren’t meaningless as the vast majority agreed that some degree of fear for reinjury was at play.
Certainly, not all these clients needed psychological assistance. However, what they did need were opportunities to decide whether those fears needed specialist attention. By far, most never considered that their fears could at least contribute to their reduced range of motion. Once they learned about the possibility, many – if not most – were able to reframe their relationships with their fears, and therefore their physical concerns.
I believe that for us here at Advaya there’s only one success metric worth measuring. This is the number of clients that could be helped successfully, within minimal time, to make them fully independent from therapeutic assistance – ours, or of that of any other therapist. Leaving Psychological Points of Bind out of scope when working with clients may be good for business economically, especially when it prompts them to book repeat sessions for fear of constant reinjury, but this approach doesn’t gel with the intentions I once set for our practice.
That we’ve always taken skeletal, tissue, and psychological Points of Bind perhaps more serious than most other clinics may explain why our small practice continues to grow constantly. Even if the existence of Psychological Points of Bind remains scientifically disputed among medical, therapeutic, and clinical specialists I will continue to believe that clients should be made aware of it, at least as a concept for exploration.
This Journal aims to start those conversations. I welcome your thoughts, comments, critiques, and questions below.
Comments & Questions
We love to receive your comments and questions on this journal, as long as they do not contain SPAM and are constructive, polite, and aligned with the topic. You may use an alias if you wish to remain anonymous. Your email address will NOT be displayed publicly – we use it ONLY to notify you when someone else comments on your submission. Your comments and/or questions will be moderated before they become publicly visible.





























Mondi, likely to yet again ruffle some feathers among other therapists and I love that you’re doing it. As a psychologist I absolutely agree with your text. Well done. That grey area you talk about really exists because psychologists are indeed not trained or licensed to help clients with their physical body. Let’s have a chat about this one day soon? I’ll send you a PM.
Fear for reinjury?! After a ski accident twenty year ago (four injured vertebrae) I have lived with it ever since. So, if a claim needs to be made for the existence of that Psychological Point of Bind scenario, I will be right behind that. And NONE of the therapists or specialists I have seen over the years EVER spoke with me about it.
Awesome post (Journal). Thanks for putting it up Mondi!
Shame I don’t live closer to where you are Mondi (Canada) here). I’ve been reading your Journals for a while now, and this is one I just (finally) had to respond to. I KNOW that my fear of reinjury as you call it just simply freezes me. My back would be so much better if i could find a therapist who would take that more seriously. If I could jump on a plane to come see you I honestly would…